Thursday, April 25, 2024
This activity is intended for primary care physicians, infectious disease specialists, nurses, nurse practitioners, pharmacists, physician assistants, and other members of the healthcare team who prescribe or manage antimicrobial drugs.
The goal of this activity is for the healthcare team to be better able to evaluate the application of antimicrobial treatment for patients with COVID-19.
Upon completion of this activity, participants will:
Medscape, LLC requires every individual in a position to control educational content to disclose all financial relationships with ineligible companies that have occurred within the past 24 months. Ineligible companies are organizations whose primary business is producing, marketing, selling, re-selling, or distributing healthcare products used by or on patients.
All relevant financial relationships for anyone with the ability to control the content of this educational activity are listed below and have been mitigated. Others involved in the planning of this activity have no relevant financial relationships.
This activity was planned by and for the healthcare team, and learners will receive 0.25 Interprofessional Continuing Education (IPCE) credit for learning and change.
Medscape, LLC designates this enduring material for a maximum of 0.25 AMA PRA Category 1 Credit(s)™ . Physicians should claim only the credit commensurate with the extent of their participation in the activity.
Successful completion of this CME activity, which includes participation in the evaluation component, enables the participant to earn up to 0.25 MOC points in the American Board of Internal Medicine's (ABIM) Maintenance of Certification (MOC) program. Participants will earn MOC points equivalent to the amount of CME credits claimed for the activity. It is the CME activity provider's responsibility to submit participant completion information to ACCME for the purpose of granting ABIM MOC credit.
Awarded 0.25 contact hour(s) of continuing nursing education for RNs and APNs; none of these credits is in the area of pharmacology.
Medscape, LLC designates this continuing education activity for 0.25 contact hour(s) (0.025 CEUs) (Universal Activity Number JA0007105-0000-22-372-H01-P).
Medscape, LLC has been authorized by the American Academy of PAs (AAPA) to award AAPA Category 1 CME credit for activities planned in accordance with AAPA CME Criteria. This activity is designated for 0.25 AAPA Category 1 CME credits. Approval is valid until 11/11/2023. PAs should only claim credit commensurate with the extent of their participation.
For questions regarding the content of this activity, contact the accredited provider for this CME/CE activity noted above. For technical assistance, contact [email protected]
There are no fees for participating in or receiving credit for this online educational activity. For information on applicability
and acceptance of
continuing education credit for this activity, please consult your professional licensing board.
This activity is designed to be completed within the time designated on the title page; physicians should claim only those
credits that reflect the
time actually spent in the activity. To successfully earn credit, participants must complete the activity online during the
valid credit period that
is noted on the title page. To receive
AMA PRA Category 1 Credit™, you must receive a minimum score of 75% on the post-test.
Follow these steps to earn CME/CE credit*:
You may now view or print the certificate from your CME/CE Tracker. You may print the certificate but you cannot alter it.
Credits will be tallied in
your CME/CE Tracker and archived for 6 years; at any point within this time period you can print out the tally as well as
the certificates from the
CME/CE Tracker.
*The credit that you receive is based on your user profile.
CME / ABIM MOC / CE Released: 11/11/2022
Valid for credit through: 11/11/2023, 11:59 PM EST
processing....
Note: The information on the coronavirus outbreak is continually evolving. The content within this activity serves as a historical reference to the information that was available at the time of this publication. We continue to add to the collection of activities on this subject as new information becomes available. It is the policy of Medscape Education to avoid the mention of brand names or specific manufacturers in accredited educational activities. However, manufacturer names related to the approved COVID-19 vaccines are provided in this activity in an effort to promote clarity. The use of manufacturer names should not be viewed as an endorsement by Medscape of any specific product or manufacturer.
Antimicrobial stewardship has not always been top-of-mind during the COVID-19 pandemic, and the authors of the current study described the different forces affecting antimicrobial prescribing from 2020 to the present time. Early reports from China at the outset of the pandemic conveyed that up to half of all deaths related to COVID-19 were due to secondary infection; however, subsequent studies found rates of co-infection of SARS-CoV-2, the virus that causes COVID-19, with other organisms in 3.5% of hospitalized patients, and 14.3% of these patients developed secondary infections.
Of course, the high risk for hospitalization and mortality and lack of clear guidelines or treatment alternatives for the management of COVID-19 also contributed to antimicrobial overuse, but the authors of the current review noted that this phenomenon was most prevalent early in the pandemic and faded with time. The effect of COVID-19 on antimicrobial resistance patterns is largely unknown.
The current study by Khan and colleagues provides a review of research into the use of antimicrobial drugs during the COVID-19 pandemic.
A statement by the Society for Healthcare Epidemiology of America (SHEA), published online on September 14 in Infection Control & Hospital Epidemiology,[1] offers healthcare providers guidelines on how to prevent inappropriate antibiotic use in future pandemics and avoid some of the negative scenarios that have been seen with COVID-19.
According to the US Centers of Disease Control and Prevention (CDC),[2] the COVID-19 pandemic brought an alarming increase in antimicrobial resistance in hospitals, with infections and deaths caused by resistant bacteria and fungi going up by 15%. For some pathogens, such as the Carbapenem-resistant Acinetobacter, that number is now as high as 78%.
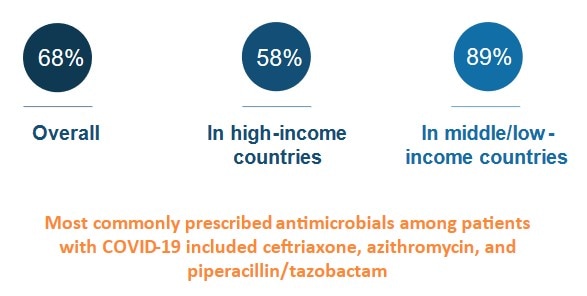
The culprit might be the widespread antibiotic overprescription during the current pandemic. A 2022 meta-analysis[3] revealed that in high-income countries, 58% of patients with COVID-19 were given antibiotics, whereas in lower- and middle-income countries, 89% of patients were put on such drugs. Some hospitals in Europe[4] and the United States[5] reported similarly elevated numbers, sometimes approaching 100%.
"We've lost control," Natasha Pettit, PharmD, pharmacy director at University of Chicago Medicine, told Medscape Medical News. Pettit was not involved in the SHEA study.
"Even if CDC didn't come out with that data I can tell you right now, more of my time is spent trying to figure out how to manage these multi-drug-resistant infections, and we are running out of options for these patients," added Pettit.
"Dealing with uncertainty, exhaustion, critical illness in often young, otherwise healthy patients, meant doctors wanted to do something for their patients," said Tamar Barlam, MD, an infectious diseases expert at the Boston Medical Center who led the development of the SHEA white paper, in an interview with Medscape Medical News.
That something often was a prescription for antibiotics, even without a clear indication that they were actually needed. A British study[6] revealed that in times of pandemic uncertainty, physicians often reached for antibiotics "just in case" and referred to conservative prescribing as "bravery."
Studies have shown, however, that bacterial co-infections in COVID-19 are rare. A 2020 meta-analysis[7] of 24 studies concluded that only 3.5% of patients had a bacterial co-infection on presentation, and 14.3% had a secondary infection. Similar patterns had previously been observed in other viral outbreaks. Research on MERS-CoV,[8] for example, documented only 1% of patients with a bacterial co-infection on admission. During the 2009 H1N1 influenza pandemic, that number was 12% of non-intensive care unit (ICU) hospitalized patients.
Yet, according to Pettit, even when such data became available, it did not necessarily change prescribing patterns.
"Information was coming at us so quickly, I think the providers didn't have a moment to see the data, to understand what it meant for their prescribing. Having external guidance earlier on would have been hugely helpful," she told Medscape Medical News.
That is where the newly published SHEA statement comes in: It outlines recommendations on when to prescribe antibiotics during a respiratory viral pandemic, what tests to order, and when to deescalate or discontinue the treatment. These recommendations include, for instance, advice to not trust inflammatory markers as reliable indicators of bacterial or fungal infection and to not use procalcitonin routinely to aid in the decision to initiate antibiotics.
According to Barlam, one of the crucial lessons here is that if physicians see patients with symptoms that are consistent with the current pandemic, they should trust their own impressions and avoid reaching for antimicrobials "just in case."
Another important lesson is that antibiotic stewardship programs have a huge role to play during pandemics. They should monitor prescribing and also compile new information on bacterial co-infections as it gets released and make sure it reaches the physicians in a clear form.
Evidence suggests that such programs and guidelines do work to limit unnecessary antibiotic use. In one medical center in Chicago, for example, before recommendations on when to initiate and discontinue antimicrobials were released, over 74% of patients with COVID-19 received antibiotics. After guidelines were put in place, the use of such drugs fell to 42%.
Pettit believes, however, that it is important not to leave each medical center to its own devices.
"Hindsight is always twenty-twenty," she said, "but I think It would be great that if we start hearing about a pathogen that might lead to another pandemic, we should have a mechanism in place to call together an expert body to get guidance for how antimicrobial stewardship programs should get involved."
One of the authors of the SHEA statement, Susan Seo, reports an investigator-initiated Merck & Co., Inc. grant on cost-effectiveness of letermovir in patients with hematopoietic stem cell transplant. Another author, Graeme Forrest, reports a clinical study grant from Regeneron Pharmaceuticals, Inc. for inpatient monoclonals against SARS-CoV-2. All other authors report no conflicts of interest. The study was independently supported.
Figure. Use of Antimicrobial Agents During Infection With COVID-19
|
Implications for the Healthcare Team The healthcare team should continue good stewardship practice to prevent the inapproriate use of antimicrobial drugs during the COVID-19 pandemic. |