Quinn Capers IV, MD, a professor of cardiovascular medicine and vice dean for faculty affairs at The Ohio State University has long advocated for increased diversity in medicine and for physicians to be activists.
As protests broke out across the globe in response to the killing of George Floyd, Capers sent out a tweet to inspire Black boys who want to be doctors, but may lack visible role models.
Medscape caught up with the interventional cardiologist. Our original interview was conducted before the recent controversy over a paper in the Journal of the American Heart Association that argued against affirmative action and was eventually retracted. Capers has submitted a rebuttal to that paper, and addresses the issue below.
This interview has been edited for length and clarity.
Let's start with the epic tweet — your message to Black boys who want to become physicians. Why did you send out that tweet that day?
Quinn Capers IV, MD: With everything that's going on in the country over the last two months, my mind went to the fact that our physician workforce does not come close to reflecting the diversity in this nation.
Some of that is because of racism and social determinants of success, things that keep people back and make them feel discouraged. Seeing the unrest coming out of the acts of police brutality, and racism, and also the disproportionate burden on communities of color of COVID-19 in terms of hospitalizations and deaths, I wanted to send a hopeful message.
Because it's been a tough time to be Black in America. I used my story to send a message of hope and encouragement for others.
When you were growing up, were there mentors who helped you believe that it was possible to become a doctor?
I got tremendous support from my loved ones, from my mother and my sister. I also had a cousin who wanted to go into healthcare and every time we met, she and I would encourage each other.
A few school teachers were very proud of me and I really basked in the glow of their pride. But in terms of a physician, or even a medical student or resident, somebody that I could look to, I did not have that.
But I was always an avid reader and I loved history, particularly black history. So I guess you would say that I had many virtual mentors, people I was reading about who were inspiring me.
But there was not a human physician to encourage me. That's one reason why I try to do a lot of mentoring. I try to be for people what I never had because I know how important that is.
In one of your TedX Talks at Ohio State , you spoke of the importance of being an activist and a physician. Why do you think that's important?
I think it's part and parcel of the spirit of wanting to be a physician. People go into medicine because they want to help, they want to relieve suffering, they want to prolong life.
And as I said, in one of my TED Talks, that in itself is a little bit revolutionary. Because if the natural state of things is that people grow old, get sick and die and you want to interrupt that, to slow that down, that is a revolutionary act.
Beyond that, for us to really do the best we can for our patients, we have to do more than simply pay attention to the patient in front of us during an office visit, or for me when I'm in the cath lab, or the patient that we see when we go on rounds
While we can be successful with writing the right prescription, and doing the correct procedure, and healing them in the moment, there's so much more that goes on with their lives. We are doing an incomplete job if we aren't also an activist trying to promote better policies that are more equitable, and just.
This includes advocating for people to vote, advocating for fair and just policing, advocating for clean air, clean water, things like that. As physicians, we want to heal our patients, but it's just as natural, in my opinion, for physicians to also be activists who want to heal society, especially given what's happening in the country now.
Are you hopeful that there will be some meaningful change?
I am. This is not the first time that racism has really exploded on the national scene. This is not the first time that we've had a series of unarmed black and brown people that were killed by police officers in a way that seems to be fueled by racism and bias. But what is different this time, is that the whole world seems to be fed up with racism. With some of these earlier police killings, I don't remember the protests going international and global.
When I see demonstrations in Amsterdam, in Iran, in Italy, and they're holding signs of George Floyd, I get the impression that this is something different. Now, all 50 states in the US, plus many countries around the globe, seem to be coming together with one voice to say, this is wrong. We need change and we don't need it tomorrow, we need it now.
You've noted that Ohio State is one of the most diverse medical schools in the country. What are the keys to that?
I'm proud to say that we've been in the top 10 for the last 3 years, according to US News and World Report . A reporter scours the AAMC data for the top 10 majority schools with the most African American students. They exclude the historically black medical schools — Howard University, Meharry, Morehouse, and Charles Drew — which leaves about 150 majority race medical schools. Last year, we were number two in the nation. This year, we're tied for number four.
How we got there was by thinking of diversity as central to being an excellent institution. When I was a dean of admissions, one of the first things I did was work with other stakeholders to develop a mission statement for admissions: What are the traits that we want to see in OSU College of Medicine students?
One thing that came through loud and clear was that we considered diversity a necessary ingredient in our student body. We wanted that. We put the mission statement on a large placard that sits in all of our admissions committee deliberation sessions.
Ohio State admissions committee Mission Statement
Then we set about making structural changes that would allow us to move closer to being more diverse. One of the first things we did was adopt the concept of holistic review, espoused by the AAMC. We were one of the first medical schools to have the onsite, holistic review workshop. This was a new way of looking at medical school applicants that put the academic record in its proper place.
The academic record used to have such an outsized role: if you were not a nice person, someone who did not demonstrate compassion for your fellow man, but you got really good grades, you would get into medical school. The holistic review values the academic record, but it puts it in perspective and on an equal footing with the experiences and the personal attributes of the student.
When we adopted the holistic review, our diversity increased. The other thing we did that was a little more cutting edge was that we started thinking about unconscious biases. Because of our past experiences, we might unknowingly associate certain demographic groups with either negative or positive attributes.
I started thinking about this in 2012, and decided to study it. We found that the majority of our admissions committee have what we call implicit White race preference, which means when they look at a White person's face, they automatically associate it with positive things. And when they look at a Black person's face, they unconsciously associate that face with negative concepts.
With that information, we began training to override implicit biases. We've now made implicit bias training an annual requirement to be on our admissions committee. After we did implicit bias mitigation training, the very next class that we admitted was the most diverse class ever.
We published this in 2017 and showed that you can be trained to overcome your implicit biases, and this can help you interact with people in different ways that result in schools enhancing their diversity.
By diversity, we mean diversity of race, ethnicity, gender, sexual identity, and just as important, of thought. We don't want 200 students (our class size) who think exactly alike. We want this nice gumbo of people who have different backgrounds, races, religions, ethnicities, different ways of looking at the world, because it helps produce physicians who are more well rounded and who feel more comfortable treating diverse patients.
Those are some of the concrete things that we've done to enhance our diversity.
Did you use Implicit Association Tests?
Yes. We use Implicit Association Tests every year. We've got a pretty big committee, about 140 people, and we had all of them take three of the IATs: the race attitude test, the gender career stereotype test, and the sexuality bias test.
We haven't published this yet, but we found that 50% or more of our committee unconsciously associate woman with homemaker. They look at a man and unconsciously associate the man with career.
At our annual retreat, we talked about the aggregate results and then we went right into a discussion about how to overcome or override these implicit biases.
Is there any concern given cancel culture that if it became public that, say, Professor so-and-so failed his implicit bias test, that information might be used to get rid of him?
People ask that question occasionally. That is the wrong way to think about implicit bias. Remember, implicit bias is unconscious. It is simply your brain's integration of all these stimuli that you've seen your whole life.
Let's take me as an example. If I'm looking at the news, and it's showing violent crime, many times they're showing me pictures of young black men. Then I watch fictional movies and the criminal roles are played by young black men, or I read books about violence and crime that feature young black men. My unconscious brain will put that together to say, 'young black man' equals violence.
That is not showing any bad characteristics or traits of me. That is just my brain doing what it is supposed to do. It would be wrong to take any kind of punitive action against anybody because of their implicit biases.
The right way to use implicit bias testing, or workshops, is to take the approach that this is how the brain works. We all have these implicit associations that can be helpful, but at times can be harmful. So let's talk about how we can override them.
And by the way, every time we've done this, it was all anonymous because of what you just said. We don't want somebody saying, "Oh, Professor Jones has implicit gender bias or implicit, elderly bias so let's not have him on the committee."
You wrote a paper with cardiologist Claire Duvernoy, MD about the roadblocks to the inclusion of people from different backgrounds using some case studies. What do you want people to take away from that paper?
What we hope they take away from that is that there are many reasons why we don't have diversity in our profession. I'm now specifically talking about cardiology. Some of it has to do with the lack of good advice, and a lack of mentoring. We walk through a few case studies. You might remember the African American male who did not have an advisor to tell him, 'Listen, if you want to do cardiology, then as a resident, you need to do some cardiology research.' He didn't find that out until later, because he didn't have a mentor.
There's evidence to show that White males are the most likely people to be mentored. They are the group that senior persons will most likely reach out to and say, 'I want to mentor you.' What that means for women and for people who aren't White males is that instead of sitting and waiting for somebody to tap you on the shoulder, we've got to be aggressive and maybe make the first move.
It doesn't have to start with asking, Will you be my mentor? That's a big ask. But you could say 'I'm looking for a project to work on. Do you have any suggestions?' And then once you have a connection, ask questions. Then maybe you make another request and it'll kind of happen organically.
One of the things I want people to get is that if you sit back and wait for somebody to knock on your door and say, 'Hey, I want to mentor you,' you might lose out.
Could there be more virtual mentoring, if there are, say, no people of color or women at your institution?
Absolutely, given that almost all of our meetings are virtual now. I've also found social media to be a good way to reach out to people. A mentor typically checks in with you at different times, and sets expectations: 'I'll check back with you in two months and here are some things that you should have done.'
There's no reason why that cannot be done virtually. We've had some attempts at virtual mentoring of pre-med students, residents and fellows, that were very positive.
Recently on Twitter, the American College of Cardiology, Fellows in Training group put out some advice for the upcoming fellowship interview season (which will be virtual) so that's an example of mentoring. I'm all for mentoring virtually via social media, email, text, whatever it takes.
How do you respond to critics (and we'll get some in the comments) who roll their eyes when issues of diversity or inclusion come up and say just hire the best people?
I think it was Jimmy Kimmel who said that the most dangerous neighborhood in the country is the Comments section of websites.
That is especially true, and I've noticed that fact if the article has anything to do with racial issues or diversity. I've been involved in several articles that are in a public forum like that. That train is never late.
It's usually something to the effect of, 'If I need somebody to operate on my heart, I don't want it to be the most diverse person. I want it to be the most qualified person.' Or If you're admitting medical students, residents, or picking the next leader of your department, the only thing that should count is merit.
And it's amazing that there is unanimity, when you ask people, 'Gee, what do you mean by merit exactly?' What they're talking about is scores on a standardized test: the MCAT, or the ACT, or the step one board exam.
There has never been any evidence that somebody who gets 90% of those questions right will be a better cardiologist or surgeon or family physician than somebody who gets 80% of those questions correct. So when they say I just want the best, they're clinging to a metric that doesn't measure who is the best.
Maybe if you're choosing mathematicians, you could say, whoever scores highest on this math test is the most qualified to be a mathematician. But not in medicine.
There is no objective justification for saying that the person who scored the best on a standardized test is the best person to be admitted to medical school, or residency or fellowship. Maybe the person who got 80% of the questions correct is better able to connect with me as a patient or is better able to problem solve if I'm not getting better. Then that person is the better doctor.
"High test score equals best doctor" was the cornerstone of the controversial paper Diversity, Inclusion, and Equity: Evolution of Race and Ethnicity Considerations for the Cardiology Workforce in the United States of America From 1969 to 2019 . What do you say to those who see the paper's retraction as an example of political correctness gone amok?
The article was not retracted because the author's views are controversial or hurt people's feelings. The bar for retraction is that that author falsified data. That bar was met. This is an example of editors being made aware of deliberate falsification and taking the appropriate step.
The journal should be commended. They made a mistake. They acknowledged the mistake, apologized, retracted the article, and will publish the rebuttal.
I believe that all major journals should have an Associate Editor for Diversity, Equity, and Inclusion tasked with scanning all submissions for signs of racism, or other "isms." This paper illustrates the need for more diversity and more research. Let's get to work creating a database so large and irrefutable that it will be much easier to refute the next attack on affirmative action.
When you spoke with Bob Harrington, MD, last year about the medical school pipeline, you said there wasn't help coming soon in terms of diversity. Do you think the increased use of NPs and PAs and those shorter training times could help get more diversity in the medical space sooner?
We need diversity in all of the allied health professions. Medicine is a team sport now, but the physicians are the leaders of the team so we definitely need diversity among physicians. And we need diversity among nurse practitioners, physician assistants, respiratory therapists, pharmacists, etc.
If what you're asking is are some of those careers perhaps more attractive because of shorter training times? I think they could be. But because I work at a medical center that has a nursing school, a pharmacy school, and a dental school, I know they'll tell you that they're lacking diversity as well.
I actually think it would be unfortunate if people who dreamt of becoming a physician said, 'Well, instead of being a physician, let me choose one of these other professions because the time to get there is shorter.' That's not what we're hoping for.
What we're hoping for is that we can all get kids excited about healthcare. Some of them will want to be physicians, some will want to be a physician assistant, some will want to be a nurse or nurse practitioner. There's room for everybody.
What can people do, starting today, to make that a reality?
Be visible as a role model, whether you're working in private practice or in academic medicine. There's somebody that looks up to you. Reach out to people.
When I was in school, I loved Career Day. And now as a working professional, I love being on the other side of Career Day and talking to youngsters about what I do. I do that at my church, I do that just about every opportunity that I get. That's the easy stuff that we can all do.
Some people get frustrated, and think one session with a pharmacist during kindergarten to high school is not going change much. I disagree. While it might not do much for everybody sitting in that classroom, there will be one kid who will be on fire after listening to you.
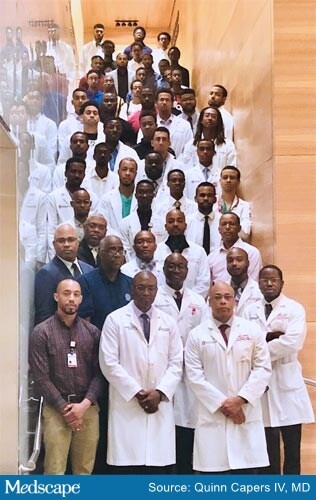
I think that's critically important and we can do it through social media. About three years ago, as I mentioned on the podcast with Bob Harrington, some Black physicians on Twitter (myself included) decided to start the hashtag #BlackMenInMedicine to promote images of black male physicians and to inspire.
This really was a national effort in response to AAMC data showing that the number of black men applying to medical school is dropping.
Another thing that people can do is help spread the idea of the importance of inclusion, diversity, and inclusion as a marker of excellence, wherever you work. Diversity equals quality and there's evidence for that. There's evidence that diverse groups tend to make better decisions, and that diverse physicians tend to increase healthcare for all. Read those papers, help to write those papers, help to generate data and spread the word.
Is there anything else you want to add?
Just to say that this is a really important time in our country's history, and really in world history, in terms of racism and bias. There's a global call to end racism now, today. Medicine needs to heed that call. There's a lot of racism and bias in medicine so medicine needs to get its house in order to become a force for good in the fight against racism.
Tricia Ward is an executive editor at Medscape who primarily covers cardiology and nephrology. She is based in New York City. Follow her on Twitter @_triciaward.
For more from theheart.org | Medscape Cardiology, join us on Twitter and Facebook
Medscape Medical News © 2020
Cite this: Diversity, Not Test Scores, Equals Quality in Medicine: An Interview With Quinn Capers IV, MD - Medscape - Aug 17, 2020.











Comments