Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I'm Dr F. Perry Wilson of the Yale School of Medicine.
The Centers for Disease Control and Prevention (CDC) recommendations for who should get an Omicron booster are very straightforward: everyone, basically, if they are over age 12, at least 2 months out from their original vaccine series or most recent booster shot, and at least 90 days out from a COVID infection. This makes a significant majority of Americans immediately eligible for an updated booster.
But, for many Americans, the CDC advising something is not the most compelling argument to do it. You can take this as a sad commentary on the loss of faith in science and public health, or the inexorable result of poor messaging from government agencies.
But the truth is, there are good arguments to get the updated booster. There are even some decent arguments not to get the booster. To me, though, all the hot takes boil down to just two positions. Let me walk you through it.
First of all, I would like to dispense with the line of argument that suggests this updated vaccine poses significant risk to the population. It is true that, while human trials are ongoing for the authorized BA.4/BA.5 bivalent vaccine, we have not seen data regarding safety or efficacy. Those who are skeptical of the vaccination program point to the lack of data on human efficacy and safety as a major red flag. It makes for some nice headlines, for sure, but honestly these arguments are simply not that compelling to me.
The formulation of the updated booster is essentially identical to the former booster, with the substitution of small bits of RNA sequence to make the spike protein the mRNA generates look more like the Omicron spike protein. And I'm not terribly worried that that change is going to increase the safety risk because tons of people — hundreds of millions of people — have been exposed to that spike protein already. They just got it via infection. There is no compelling biological argument how this vaccine could be more dangerous than Omicron infection itself.
So yeah, I think the safety argument is a bit too convenient. If I'm being honest, I find it a bit disingenuous.
No, the good argument to not get the bivalent booster is an efficacy argument. We don't know how good it will be at protecting people. Human data from the BA.1 vaccine trials show an increase in anti-Omicron neutralizing antibody production compared with the standard booster.
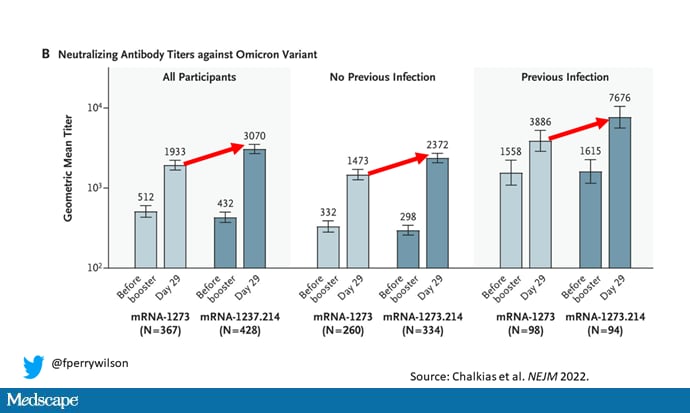
But of course, the booster at your local pharmacy is not the BA.1 booster; it is the BA.4/BA.5 booster. We know the booster works pretty well in mice, but humans are not nearly as cute.
Moreover, it is clear that the booster will have different efficacy in different people.
The CDC wanted its recommendations to be simple. But there's no reason for us to be simple here. We can appreciate that if you were infected with the Omicron variant, you are likely more protected against the Omicron variant than if you were never infected or infected with a prior variant.
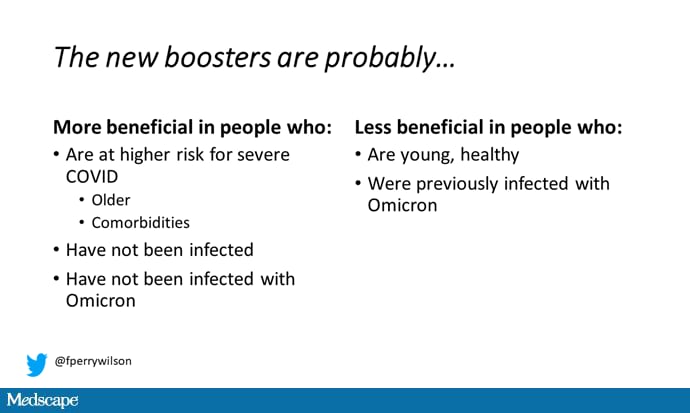
We can appreciate that the risk for infection differs on the basis of patient factors like age and comorbidities. But those conversations, best had between a patient and a doctor, are too nuanced for CDC messaging. I don't blame the CDC for trying to keep things simple. But if you want to convince yourself that the booster won't help you specifically, you have quite a few avenues — and you may be absolutely correct.
There's something of a philosophical reason to get the new booster, regardless of your risk for severe disease, though.
A hypothetical: If we all got vaccinated with this booster, I really do think it would have a significant impact on the pandemic overall. It might not help me that much, but if we really all did it, the virus would have far fewer safe harbors to jump into, maintain its presence, and further mutate. But as of right now, just about one third of people in the US have gotten any booster (34.9% of those aged 5 or older— or a total of 109,201,576 — got a first booster dose).
That's not all of us. There's thus a moral hazard here: Why should I get this booster if it won't contribute to the overall state of the pandemic, particularly if I don't think I'll get significant health benefits personally?
Immanuel Kant would tell us that we should get the booster anyway because we should choose to act in a manner such that, if everyone acted that way, the world would be a better place — that's the categorical imperative. But society today is not terribly Kantian. So maybe moral philosophy isn't the best reason to get this booster.
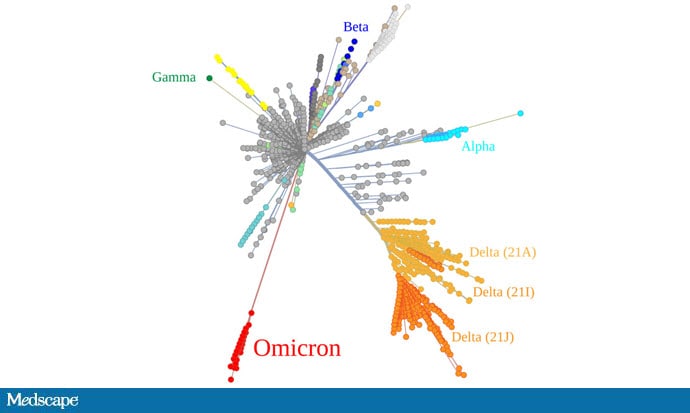
But there is one argument that I find particularly compelling. It is simply this: The next variant of SARS-CoV-2 is likely to be more closely related to Omicron BA.4/BA.5 than any other variant.
In other words, the reason to get boosted with this particular booster is not because it will protect you against the current coronavirus wave (after all, more than half of Americans got infected with it already). It's that it's a reasonable guess — the best guess, probably — as to what the next variant will be.
Updated vaccines should anticipate the next variant of the virus. We get the flu vaccine in anticipation of the upcoming flu season, on the basis of data from parts of the globe where flu strikes earlier. We don't have that data with pandemic SARS-CoV-2, but if I were a betting man, I would bet that the next variant comes from Omicron, simply because Omicron has caused more infections than any other variant and is the most recent to emerge.
I could be wrong. Omicron didn't come from Delta, as this genetic lineage map shows.
But it's a decent guess, and the main reason that I'm getting my Omicron booster. Not really for Omicron, but for Phi or Omega or whatever we face next, until such time that immunity is widespread enough that the loss of life due to COVID — a rate that is still five times higher than that of endemic flu — is truly mitigated.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale's Clinical and Translational Research Accelerator. His science communication work can be found in the Huffington Post, on NPR, and here on Medscape. He tweets @fperrywilson and hosts a repository of his communication work at www.methodsman.com.
Follow Medscape on Facebook, Twitter, Instagram, and YouTube
Credits:
Image 1: New England Journal of Medicine/F. Perry Wilson, MD, MSCE
Image 2: F. Perry Wilson, MD, MSCE
Image 3: Wikimedia
Medscape © 2022 WebMD, LLC
Any views expressed above are the author's own and do not necessarily reflect the views of WebMD or Medscape.
Cite this: F. Perry Wilson. The Best Reason to Get an Omicron Booster - Medscape - Sep 21, 2022.







Comments